INTRODUCTION:
The UCL is a ligament that connects the arm bone (humerus) to the forearm bone (ulna) on the inner aspect of the elbow. It is also known as the “medial collateral ligament” of the elbow. On the outer aspect, the “Lateral collateral ligament” connects the arm and the forearm bones, and together the 2 ligaments balance (stabilize) the elbow joint.
ANATOMY:
In the elbow, two of the most important ligaments are the ulnar collateral ligament (UCL) and the lateral collateral ligament (LCL). The ulnar collateral ligament is on the medial (the inner side) side of the elbow, and the lateral collateral is on the outside. The ulnar collateral ligament is a thick band of ligament that forms a triangular shape along the medial elbow. Together these two ligaments connect the humerus (arm) to the ulna (forearm) and keep it balanced as the elbow moves.
These ligaments balance (stabilize) the elbow. They can be torn when there is an injury or dislocation of the elbow. If they do not heal correctly the elbow can be too loose or unstable. The ulnar collateral ligament can also be damaged by overuse and repetitive stress, such as the throwing motion ( baseball pitchers, cricket players, javelin throwers)
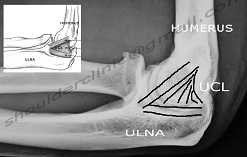
UCL is on inner side of elbow UCL is a triangular ligament connecting arm and forearm bones.
THE PROBLEM:
UCL tear is usually a sports injury; however, it may also occur if one falls on the outstretched arm.
The most common reason to develop this tear is overuse of elbow in throwing motion.
Repetitive activity results in “microtears” in the area, and healing takes place by formation of scar tissue. This tissue is abnormal, and causes instability, and ultimately, weakness and pain.
Eventually, the ligament ruptures completely.
SYMPTOMS:
PAIN:
Pain starts at the inner bump of the elbow. and can spread down the forearm.
The entire forearm may feel weak.
Swelling and/or bruising may be seen if the tear is sudden (acute).
DIAGNOSIS:
The most important thing is to first diagnose the condition correctly. Several other elbow problems may cause similar pain, and therefore an orthopaedic surgeon (elbow specialist) must be consulted.
Clinical tests can accurately diagnose the condition and also differentiate it from other problems like Golfer’s elbow, ulnar nerve problems, etc.
Xrays are important, and will somtimes show a small piece of bone that may be pulled off with the ligament.
MRI should always be done to show the complete picture and to confirm the diagnosis.
TREATMENT:
In some cases, the problem can be completely treated with medicines and physiotherapy.
Special splints or braces may be worn for temporary relief.
Many athletes are able to return to play without further treatment. If conservative (nonoperative) care does not change the picture, then surgery may be needed.
Arthroscopy ( keyhole surgery) is used to accurately diagnose the problem, and treat associated problems. This procedure involves 2 tiny keyholes. One is used for a camera to look inside the elbow and see the condition of the joint. It may be possible to debride any tissue fragments or frayed edges. During debridement, the surgeon carefully cleans the area by removing any dead or damaged tissue. Any bone spurs or areas of calcium build-up are also removed.
A mini-open procedure is used to reconstruct or repair the ligament tear.
This involves a 2 cms skin cut, and the ligament is stitched back. In some cases (old tears), a tendon graft is obtained from the forearm or the knee, and is used to create a new ligament. This is called “Docking technique” ( also called Tommy-John surgery).
Surgery is advised only when all other modalities have been tried and have failed.
Surgery is effective, and complete recovery iin 4-6 months.
Rehab is necessary in the postoperative period for early recovery.