INTRODUCTION:
TFCC is an acronym for triangular fibrocartilage complex. TFCC is an important ligament on the ulnar side ( little finger side) of the wrist, and helps to keep the wrist balanced. Milber injuries of TFCC are often called “ wrist sprain”.
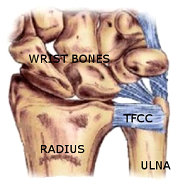
ANATOMY:
The triangular fibrocartilage complex (TFCC) connects the forearm bones at the wrist, and helps to balance them during wrist movements.. It is triangular in shape and made up of several ligaments and cartilage. The central cushion of TFCC is called the “articular disc”. Other componants include radioulnar ligaments, meniscal homologue, ulnar collateral ligament, etc. Together, these ligaments stabilize the distal radioulnar joint (part of the wrist) while improving the range of motion and gliding action within the wrist.
THE PROBLEM:
The TFCC works as a stabilizer and force transmitter across the inner side of the wrist. Traumatic injury or a fall onto an outstretched hand is the most common mechanism of injury. The hand is usually in a pronated and hyperextended position. Other tears are degenerative, and occur with minor injuries.

Falling on outstretched hand, wrist hyperextended
SYMPTOMS:
Pain starts at the inner aspect of the wrist, and may go up into the forearm.
Actions like Hoding a heavy bat/ racquet, turning a doorknob, opening a jar etc aggravate the pain.
Clicks or catching may be felt in the wrist.
Some patients have a sensation of weakness in the wrist and forearm.
The entire forearm may feel weak.
Wrist movements, and even grasping, can make the pain worse.
DIAGNOSIS:
The most important thing is to first diagnose the condition correctly. Several other wrist problems may cause similar pain, and therefore an orthopaedic surgeon (wrist specialist) must be consulted.
Clinical tests can accurately diagnose the condition and also differentiate it from other problems like ltendon / nerve problems, radioulnar joint problems etc.
Xrays are important, and will sometimes show an old fracture of the styloid (a bump on the ulna bone), or an abnormally prominent styloid (bump)


Old Fracture Abnormally prominent bump
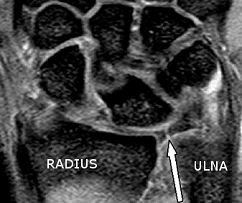
MRI may be done to show the complete picture and to confirm the diagnosis.
Acute injuries can be painfully swollen preventing proper examination. In such cases, an MRI can help to confirm the diagnosis. Sometimes, a dye is injected before the MRI to clearly show the tear. Still, the diagnosis may be missed (studies show that almost half the patients with a true triangular fibrocartilage complex tear have normal arthrograms)

DIAGNOSTIC WRIST ARTHROSCOPY is the best way to assess the tear.
A long thin needle is inserted into the joint. A tiny TV camera on the end of the instrument allows the surgeon to look directly at the ligaments. Using a probe, the surgeon tests the integrity of the soft tissues. A special trampoline test can be done to see if the fibrocartilage disk is torn. If a tear is found, it can be repaired at the same time.




TREATMENT:
If the wrist is stable, the problem can be treated with medicines and physiotherapy.
Special splints or braces may be worn for temporary relief.
Steroid injections can help to reduce the inflammation and pain., however, the effect is temporary, and sometimes it does not cure the problem.
REPEATED STEROID INJECTIONS ARE HARMFUL AND SHOULD NOT BE TAKEN.
There are other sonography guided injections (PRP, Prolotherapy, Growth factors, Bone marrow aspirate, etc), however, there is no scientific evidence to support their use. They are expensive, and may be no better than just rest and exercise.
Arthroscopic (Keyhole) release is commonly performed for TFCC tears that do not get better with non-surgical treatment. This procedure involves 2 tiny keyholes. One is used for a camera to see the tear on a TV monitor. The other hole is used to pass an instrument to repair and / or clean up the tear.
The outside of the TFCC has a good blood supply. Tears in this area can be repaired. But there is no potential for healing when tears occur in the central area where there is no performed.
Sometimes, a tendon interposition is required, especially in old tears where tissue is deficient.
Prominent ulna bone should be looked for and resected ( arthroscopic wafer resection)
Other associated tears and problems in the wrist are treated simultaneously.
Arthroscopy is advised only when all other modalities have been tried and have failed.
Arthroscopy is effective, and complete recovery is seen within weeks.
Rehab is necessary in the postoperative period for early recovery