INTRODUCTION:
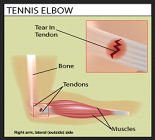
Tennis elbow (also called “Lateral Epicondititis” ) is a problem (Tendinopathy) of muscles that attach to the outer bump ( epicondyle) of the elbow.
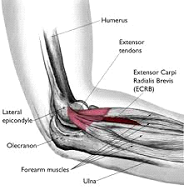
ANATOMY:
This area is also known as “common extensor origin of the forearm muscles”. These muscles go all the way upto the wrist, and help to bend the wrist backwards. Because of this wrist movement, actions that involve wrist motion ( gripping things, hitting a tennis ball in a backhand swing in tennis, etc) can transmit the load to the elbow.
The muscles involved are called “Extensor Carpi Radialis Bravis (ECRB) and sometimes Extensor digitorum (EDC)”.

THE PROBLEM:
The most common reason to develop tennis elbow is overuse of forearm muscles, and this happens in activities that involve repeated wrist movement. Any sporting activity, or even household work, can result in tennis elbow pain, and the problem is not restricted to playing tennis.
Repetitive activity results in “microtears” in the area, and healing takes place by formation of scar tissue (Tendinosis). This tissue is abnormal, and causes weakness and pain.
SYMPTOMS:
PAIN:
Pain starts at the outer bump of the elbow. and can spread down the forearm as far as the back of the middle and ring fingers.
The entire forearm may feel abnormal and stiff.
Wrist movements, and even grasping, can make the pain worse.
DIAGNOSIS:
The most important thing is to first diagnose the condition correctly. Several other elbow problems may cause similar pain, and therefore an orthopaedic surgeon (elbow specialist) must be consulted.
Clinical tests can accurately diagnose the condition and also differentiate it from other problems like ligament tears, nerve problems, etc.
Xrays are important, and will sometimes show calcium deposits in the tendons.
MRI may be done to show the complete picture and to confirm the diagnosis.

MRI shows a tear in the ECRB tendon
TREATMENT:
The problem can be completely treated with medicines and physiotherapy.
Special splints or braces may be worn for temporary relief.
Tennis elbow that does not get better even after prolonged treatment is called “refractory tennis elbow”
- Injections: Steroid injections can help to reduce the inflammation and pain., however, the effect is temporary, and sometimes it does not cure the problem.
REPEATED STEROID INJECTIONS ARE HARMFUL AND SHOULD NOT BE TAKEN. - There are other sonography guided injections (PRP, Prolotherapy, Growth factors, Bone marrow aspirate, etc), however, there is no scientific evidence to support their use. They are expensive, and may be no better than just rest and exercise.
- Sonography guided percutaneous procedures are effective, however, complications and failure of the procedure have been noted.
- Shock wave therapy: Current evidence does not support the use of this treatment method.
- Arthroscopic (Keyhole) release is commonly performed for tennis elbow that does not get better with non-surgical treatment. This procedure involves 2 tiny keyholes. One is used for a camera to see the tear on a TV monitor. The other hole is used to pass an instrument to “release” the tendon and clean up the tear.
- Other associated tears and problems in the elbow are treated simultaneously.
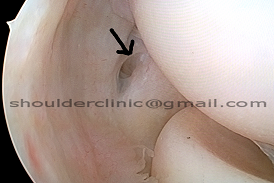
Arrow shows the tear in the tendon seen from within the elbow joint.
Arthroscopy is advised only when all other modalities have been tried and have failed.
Arthroscopy is effective, and complete recovery is seen within weeks.
Rehab is necessary in the postoperative period for early recovery.