INTRODUCTION:
S.L.A.P. is an acronym for Superior Labrum Anterior Posterior, which simply means that the attachment of the long tendon of the biceps is torn away from the upper end of the shoulder socket. (Superior Labrum=Biceps attachment, Anterior=front, Posterior=back).
ANATOMY:
The Biceps is an upper arm muscle that acts across the shoulder and elbow joints. At the elbow, it helps to bend the joint. At the shoulder, its function is more complex and incompletely understood.
The biceps has two tendons around the shoulder: the long tendon passes inside the joint via a groove in the ball and attaches to the upper end of the shoulder socket, and the short tendon passes outside the joint to an adjacent bony outgrowth (coracoid).
The attachment of the Long tendon extends to a ligament/ cartilage like structure (Labrum) which encircles the socket, thereby adding stability to this joint. The entire complex is called a Biceps anchor.

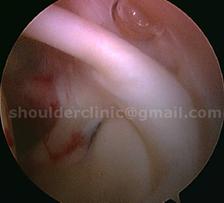
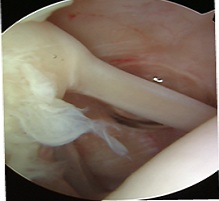
The figures show the long tendon of Biceps attaching to the shoulder socket. The hook- like passage of the tendon over the ball predisposes to SLAP tears.
MECHANISM OF SLAP TEAR:
A sudden injury to the shoulder may peel the biceps anchor off the upper socket. This is usually seen in sportsmen (throwing and rugby athletes), and sometimes in weightlifters. The hook- like passage of the tendon over the ball predisposes to SLAP tears.
TYPES OF SLAP TEARS:
Many different SLAP types have been described ranging from simple separation of the biceps anchor from the socket, to tearing away a flap from the anchor, and even extensions of these tears further to the front or back.
Type 1:
This involves mild changes (fraying) in the labrum. The labrum is not torn off the bone.

Type 2:
This type involves tearing of the labrum off the bone. This is a common SLAP injury. The entire superior labrum lifts off the bone. These tears can often be treated with physiotherapy and only sumtimes require surgery.

Type 3:
The labrum tears in a flap-like manner, and this flap resembles a bucket handle.
These tears are very painful and usually do not get better with physiotherapy. This usually requires arthroscopic surgery, where the flap is removed and the labrum is repaired back to the bone.

Type 4:
Here, the labral tear extends into the biceps tendon. These are also very painful, and almost always require surgery to resolve the symptoms.


DIAGNOSIS:
1. Clinical: Usually patients complain of pain around the shoulder that is poorly localized. Painful “popping” or “clicking” can occur.
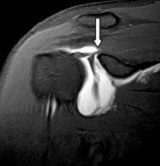
2. Radiological: SLAP tears can be visualized on MRI scans, however, the diagnostic accuracy is poor.
3. Arthroscopic: Arthroscopy accurately identifies the tear. The tear can be classified and treated based on standard recommendations in scientific literature.

ASSOCIATED PROBLEMS:
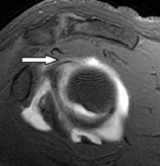
1. Some SLAP tears are associated with GANGLION CYST formation. Cysts are fluid filled swelling that can compress a nerve (suprascapular nerve) close to it and causes severe shoulder weakness and burning pain. The cyst should be decompressed arthroscopically and the tears should be repaired to prevent reccurrence.


2. PASTA tears: These are partial tendon tears that may be associated with SLAP tears. They are commonly seen in Raquet sport players. They cause severe pain while hitting the ball overhead or while throwing. High grade PASTA tears should be re-attached simultaneously with SLAP repair.


TREATMENTS OF SLAP TEARS:
These tears may be treated without surgery; however, activity modification, with avoidance of sports that need overhead arm movements, is necessary. Recovery is unpredictable, as even certain daily activity movements may stress the tear, thereby aggravating it.
Many of these tears are only identified on arthroscopy, and should be fixed at the same surgery.
Surgical repair of the lesion is necessary in sportsmen. Arthroscopy accurately identifies these tears, and three key holes are used to insert one or two tiny absorbable screw-like devices (anchor); the sutures on these are utilized to repair the tear. Some tears may need only shaving away of the torn region, and some may need a biceps tenodesis (see section on biceps).
Postoperatively, overhead activities should be avoided in the first few weeks. Thereafter, range and muscle strengthening exercises are started. Full return to sports is possible within 3 months.
Read Dr Deepak Bhatia’s scientifc publications on this topic:
1. Bhatia DN. 2012 . Arthroscopic “Cuff sparing” percutaneous (CUSP) Technique for posterior instability repair in the beach-chair position.
Tech Hand Up Extrem Surg. 2012 Sep;16(3):173-9
2. Bhatia DN, deBeer JF, vanRooyen KS. 2007. The “Bony-PASTA” lesion: An arthroscopic technique for fixation of the partially avulsed greater tuberosity. Arthroscopy 2007;23: 786 e1-786 e6
3. Direct arthroscopy of the bicipital groove: A new technique of evaluation and treatment of bicipital groove and tendon pathology. Arthroscopic suprascapular nerve decompression at the suprascapular notch. Arthroscopy 2006;22(9):1009-1013.