INTRODUCTION:
A distal biceps rupture involves tearing of the biceps tendon at the elbow. This injury occurs mainly in middle-aged men during heavy work or lifting, and sometimes in professional bodybuilders who use steroids.
ANATOMY:
The biceps muscle has 2 attachments at the shoulder, and 2 at the elbow. One of the two elbow attachments is a prominent tendon, and attaches to a forearm bone (radius). The biceps muscle moves (flexes) the elbow and gives shape to the arm.
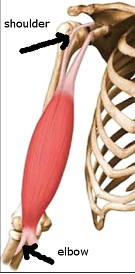
Arrows show the attachments of the biceps tendon
THE PROBLEM:
A distal biceps rupture usually happens during lifting a heavy weight with elbows bent. This forces the elbow to straighten, even though the biceps muscle is working hard to keep the elbow bent. The biceps muscle contracts extra hard, and at some point, the distal biceps tendon tears where it connects to the radius (forearm bone).
Sometimes, in elderly people, the tendon has degenerated with aging, and partial tearing can occur.
SYMPTOMS:
Sudden pain with a snapping feeling is felt in complete tears, and swelling or bruising can occur.
The biceps appears to have rolled up in the arm.
The arm often feels weak with attempts to bend the elbow.
In partial (incomplete) tears, slowly increasing pain is felt with activities, and arm may feel weak. The pain often becomes nagging in nature, and may disturs sleep at night.


Rolling up of the ruptured biceps with biceps tear at the shoulder (top) or elbow (bottom)
DIAGNOSIS:
The most important thing is to first diagnose the condition correctly. Several other elbow problems may cause similar pain, and therefore an orthopaedic surgeon (elbow specialist) must be consulted.
Clinical tests can accurately diagnose the condition and also differentiate it from other causes of pain.
Sonography is usually used to confirm the diagnosis.
MRI may be done to show the complete picture and to confirm the diagnosis.
TREATMENT:
People with low activity levels can be treated without surgery, with medication and icing.
Early surgery is usually necessary in young and active people to restore biceps continuity.
Surgery should be performed as early as possible, to prevent retraction (further rolling up) of the muscle. If surgery is delayed for a long time, repair may not be possible, and reconstruction may be necessary.
Surgery can be performed open or endoscopic.
Open surgery is necessary only in late cases, if the tendon has retracted far up into the arm.
Dr Bhatia performs this surgery as a minimally invasive endoscopic procedure.
This involves 2 tiny (3mm) skin cuts to insert a camera, and to repair the biceps tendon back to the forearm bone. Tiny metal implants ( anchors, endobuttons) are used to securely reattach the tendon back. The endoscopic procedure is very cosmetic, and performed as a daycare procedure.

Endoscopic surgery for distal biceps repair.