A calcium deposit appears in one of the tendons of the shoulder. The cause is unknown and not related to injury, diet or osteoporosis. The patient most commonly affected is a female 40-50 years of age, but other age groups and males are regularly affected.
The calcium deposit is a paste-like material in the tendon and not a hard object like one would expect.
The calcium deposit accumulates in the substance of the tendon and one of the reasons for the pain could be that the fibres of the tendon are pushed apart by the bulk of the calcium. The calcium also protrudes above the surface causing mechanical impingement against the under surface of the acromion when raising the arm. Another reason for pain is that the calcium is a foreign substance and when it escapes from the tendon into the subacromial space it is recognized as a foreign material eliciting an intense inflammatory response with acute pain.

THE SYMPTOMS :
The pain can be constant and nagging and is felt in the shoulder and outside of the upper arm, at times down the arm to the hand- aggravated by elevation of the arm. Night pain is often a feature and pain is intensified when raising the arm. In some instances the pain as well as tingling of the arm and fingers is experienced and may lead the treating physician think of the diagnosis of a nerve lesion of the neck.
Some patients experience attacks of excruciating pain, which then abate to a lower level after a few days.
ACUTE ATTACKS :
An attack of pain with an extreme intensity lasting for a few days occurs at times. During this attack, pain is constant and no movements of the arm are possible. The pain is due to the body absorbing the calcium and the process of absorption is accompanied by intense inflammation causing the pain.
After a few days the pain improves when the calcium has been absorbed- an X-ray taken at this stage will show that a previously evident deposit would now have disappeared.
THE CAUSE OF CALCIFIC TENDONITIS IS KONWN : it is not due to a faulty diet, not due to injury or overuse and not related to osteoarthritis or osteoarthritis.
SPECIAL INVESTIGATIONS : X-rays usually demonstrate the calcium deposits in the rotator cuff but the clinician should ensure that adequate views are taken in different rotations to avoid the bone overlying the deposit and making it less visible.

Natural history (the outcome) of calcium deposits in the tendons of the shoulder The calcium in the tendon can be absorbed spontaneously and this process is usually accompanied by severe pain. In these cases the intense pain lasts for a few days and then abates – if an X-ray is then taken after the attack it is noted that the calcium deposit has disappeared. It may take many years before it happens and there is no way to tell when it will occur. In other cases it will absorb over many years.
OUE MANAGEMENT OF CALCIFIC TENDINITIS :
Conservative management with physiotherapy, anti-inflammatories and pain-killers may be successful and may be continued as long as the pain is bearable.
CORTISONE INJECTION :
Can alleviate the pain, but does not absorb the calcium. It is very helpful for many patients as a first line treatment and we favour the use of a cortisone injection as initial management, due to the relatively good success rate.
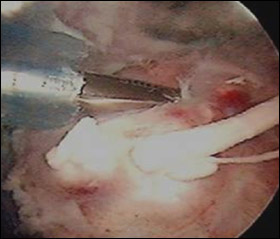
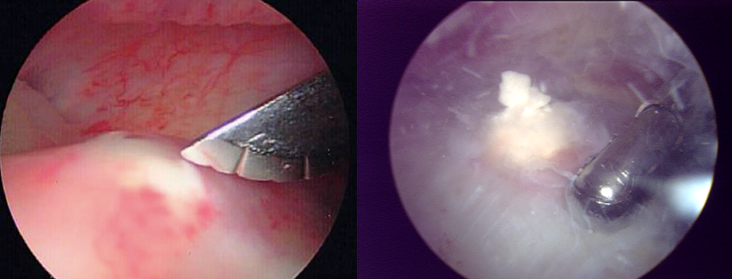
NEEDLING PROCEDURE :
With ultra-sound control and using local anaesthesia one or two (fig. 6 and 7) needles are inserted into the calcium deposit and the calcium is flushed out using sterile Saline solution. This procedure is sometimes painful and is associated with certain risks and complications.
Surgical Removal The operation becomes indicated when the patient suffers over a long period and the quality of life is affected, in other words she cannot live with the condition, and the other methods like needling have failed. Surgery also becomes indicated in some patients who have a “needle phobia” and do not want the needling procedure.
Arthroscopy (“keyhole surgery”) is done in the operating theatre. A small incision is made in the tendon under arthroscopic control and the calcium removed. Care is taken to ensure that the calcium has been completely removed at the end of the procedure by doing an X-ray in theatre. In some instances, the defect resulting from the removal of the calcium is large enough to warrant repair (closing the hole with sutures) . This is also done arthroscopically at the same time.
AFTER THE OPERATION :
The calcium can be removed totally, usually resulting in a cure, however, in a number of patients total pain relief can take up to 6 months. The reason is that the calcium leaves a defect in the tendon after removal (if large, we will repair it arthroscopically). One also has to realize that the tendon is “sick” due to the calcium which has been present in the substance of the tendon for so long. Also, some small flakes of calcium may remain in the tendon after the removal which are too small to visualize – these are absorbed over time.
This defect takes time to heal but the eventual outcome is good in all cases.
In a number of patients (30%), frozen shoulder may develop after the procedure – this means that the shoulder becomes painful and stiff. The implication is merely that it retards full recovery. The reason for the frozen shoulder is largely unknown, but patients with calcific tendonitis are the same group that is prone to frozen shoulder – mostly middle-aged ladies. It may well be due to the fact that calcium is a highly irritating substance to the joint resulting in an intense inflammation, fortunately of a temporary nature. The frozen shoulder always recovers after a few months.
POST-OPERATIVE ACTIVITIES :
Full motion and activities will be permitted immediately, within pain limits. A shoulder sling is optional, only to alleviate discomfort. In the exceptional cases where the defect had to be repaired, it will take longer.
RETURN TO WORK AND SPORTS :
Within a few days depending on the discomfort – no damage would be done through activity, in other words the resumption of activities depend on the discomfort only.
COMMONLY ASKED QUESTIONS ABOUT CALCIFIC TENDINITIS :
Q: What causes calcific tendonitis?
A: We still do not know. There is evidence that the oxygen concentration and blood supply to the tendon may be decreased. It is certainly not related to diet, osteoporosis, exercise or injury.
Q: What symptoms do I get with this condition?
A: The pain can be constant and nagging and is felt in the shoulder and sometimes down the arm/hand. It is made worse by elevating the arm. Some patients also have excruciating attacks of pain, which then abate to a lower level after a few days. The calcium can spontaneously absorb and this process is associated with severe pain.
Q: What does a cortisone injection do?
A: It helps with the pain for a short term basis but it does not take away the calcium.
Q: How many injections can I have?
A: Most doctors would say a maximum of three. There is in fact no absolute maximum, especially if they are spaced weeks or months between the injections. However, if you need a lot of injections, then this is a sign that something definite ought to be done about it.
Q: Apart from surgery, are there any other treatments available?
- Non steroidal anti-inflammatory drugs.
- Subacromial injection of steroid.
- Physiotherapy.
- Needle aspiration and irrigation.
- Extracorporeal shockwave therapy.
Q: Can physiotherapy help?
A: The physiotherapist can help you to maintain the range of motion. Some patients also find therapeutic ultrasound to be of benefit. However, the evidence that it works is conflicting. The Cochrane Musculoskeletal Database Review of 26 trials found that both ultrasound and pulsed electromagnetic field therapy resulted in significant improvement in pain compared to placebo. However, a further meta-analysis of 35 randomised controlled trials found that only 2 studies supported the use of therapeutic ultrasound over placebo. The remaining 8 showed that therapeutic ultrasound is no more effective than placebo.
Q: What is Extracorporeal shockwave therapy?
A: Extracorporeal shock wave therapy utilises acoustic waves (sound waves) to induce fragmentation of the calcium crystals. It is the same technology used to break up kidney stones.
Q: Would you recommend Extracorporeal shockwave therapy to?
A: Although this is used in some places, we do not recommend it. The recurrence rate following Extracorporeal shockwave therapy is relatively high and some patients also find the procedure quite painful and can develop troublesome haematomas (blood blisters) on the skin afterwards.
Q: What is needling?
A: Needling refers to needle aspiration and irrigation. The aim of this procedure is to drain a substantial portion of the calcium deposit; thereby stimulating the body’s cell mediated resorption. It is associated with certain risks and complications and we do not recommend this procedure routinely.
Q: Is needling suitable for everyone?
A: No. Certain patients may become acutely painful after this procedure and surgery is then necessary to evacuate the residual calcium. We evaluate each patient on an individual basis to determine who is a suitable candidate for the needling procedure.
Q: What does the actual operation to remove calcium entail?
A: It is usually done under a general anaesthetic. Using an arthroscope (keyhole surgery), the calcium is removed from the tendon. We take an x ray in theatre to make sure all the calcium is removed. Sometimes, we also have to repair the tendon at the same time if the defect left by the calcium is significantly large.
Q: How long does it take to recover from surgery?
A: Total pain relief may take up to 3-6 months. There is certainly no formal restriction on when you can return to work or do leisure activities.
Q: What is the rehabilitation like after surgery?
A: Full motion and activities are permitted immediately, within pain limits. The physiotherapist will demonstrate the exercises.
Q: Are there any serious complications with surgery?
A: The most common complication is stiffness (approx 30%), sometimes referred to as Frozen shoulder. This is also more common in patients with diabetes and middle-aged ladies. If it does occur, it does not mean that further surgery is necessary. It just means the recovery may take a little longer.
Q. Is acromioplasty (shaving of the undersurface of the acromion bone) necessary when the surgery is done for the calcium deposits?
A. Usually not, except if the surgeon notices rotator cuff impingement during the operation to drain the calcium from the tendon. Impingement is not the cause of calcific tendonitis and the mainstay of the surgical treatment is the removal of the calcific deposit.
READ DR DEEPAK BHATIA”S SCIENTIFIC PUBLICATIONS ON THIS TOPIC :
Lam F, Bhatia DN, van Rooyen KS, DeBeer JF. 2006. Modern management of calcifying tendonitis of the shoulder. Current Orthopaedics. 2006; 20: 446-452.