Introduction:
Suprascapular nerve injuries have become increasingly recognized as a cause of shoulder pain and dysfunction1. Recent advances in diagnostic and surgical techniques have simplified the management of injuries of this nerve. The purpose of this article is to provide a simplistic overview of this condition for medical practitioners and patients.
Historical aspects:
Kopell and Thomson are often credited with the first description of suprascapular nerve injuries; however, the earliest mention of this condition is found in the works of André Thomas.
Anatomy of the suprascapular nerve
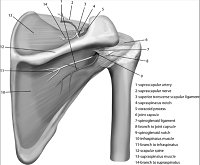
The suprascapular nerve is one of the several nerves that originate in the brachial plexus (nerves arising from the neck). The nerve passes through a small notch/tunnel in the scapula (the bone that forms the shoulder blade), and then through a second tunnel (spinoglenoid notch). Thereafter, it makes its way to the back of the shoulder. (Figure 1)Here it provides sensation to some parts of the shoulder (ligaments, bursa, AC joint), and sometimes to skin of upper arm. The main supply of the nerve is to two important muscles of the rotator cuff of the shoulder, viz. Supraspinatus, and Infraspinatus. (details in section on Rotator Cuff)
Anatomy of the suprascapular nerve Causes of injury to the suprascapular nerve
The following causes of suprascapular nerve injury have been recognized:
- Trauma: Fractures of Scapula (shoulder blade), collar bone (clavicle), shoulder dislocations, and gunshot/ stab injuries.
- Iatrogenic (during surgery): During repair of large, old tears of the rotator cuff.
- Repetitive overuse: repeated overhead use of the arm injures the nerve against the roof of the one of the two tunnels (suprascapular ligament, spinoglenoid ligament). eg, in volleyball / baseball / tennis / football players, fencers, figure skaters, dancers, weight-lifters, and hunters who use a bow,
- Tumors around the nerve may compress it, eg. cysts, abnormal blood vessels.
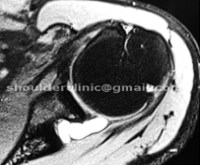
MRI of the shoulder joint shows a tumor (Cyst) compressing the nerve in one of the tunnels
Clinical presentation
The typical patient is between the ages of 20 and 50 years. The dominant shoulder is usually involved.
The main complaint is PAIN, which is dull, and the patient points to the back of the shoulder when asked to localize. The pain may increase when using the arm for overhead activities. Some patients may have little or no pain.
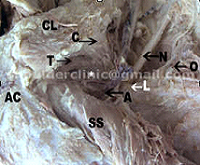
WEAKNESS and WASTING (Thinning, “withering away”) of shoulder muscles at the back of the shoulder is always present. (Figure 2). This is important to remember, as a substantial number of patients may have little, or no pain.

Arrows show wasting of the rotator cuff muscles (Supraspinatus and Infraspinatus)
How does the physician/ surgeon diagnose this condition?
The diagnosis should be SUSPECTED in any patient between 20 to 50 years of age, involved in overhead activities/ sports , or in an accident involving the shoulder (see list above), with pain and muscle wasting around the back of the shoulder.
Once suspected, the strength of the specific shoulder muscles should be tested and documented. This should be done preferably with a special instrument, eg. ISOBEX dynamometer.
A specialized muscle test, called EMG (electromyography) can confirm the injury, and can pinpoint the exact site where the nerve is injured. This is also important to assess recovery after treatment.
Imaging methods include ultrasound, and MRI (magnetic resonance imaging)
Treatment:
Suprascapular nerve injury may be treated without surgery, in some patients, by avoiding overhead activities, and rehabilitation of muscles. HOWEVER, although some patients may improve, the overall success rate is unknown, and recovery cannot be predicted.
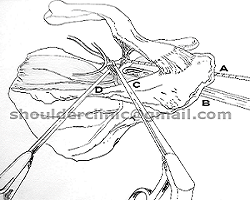
Surgical treatment depends on the cause. The specific cause is treated (eg, tumor, fracture) and the nerve is released from the tunnel that has trapped the nerve. Usually, the release is performed at the suprascapular notch (the first tunnel) and sometimes at the spinoglenoid notch (the second tunnel).
In most surgical centers, the surgery is performed OPEN, ie. by incising the skin, muscles, and surrounding tissues to gain access to the nerve.
Recent advances in arthroscopy have made this surgery possible by Endoscopic methods, ie. KEYHOLE surgery. However, at present, this technique is available only in selected centers in the world. The keyhole technique is postulated to permit better visualization of the nerve and its blood vessels, as well as the exact site of compression, thereby leading to greater accuracy in releasing the injured nerve.
Surgical release of the suprascapular nerve is associated with a high rate of pain relief and functional improvement. However, resolution of muscle wasting is less predictable.


Dr Deepak Bhatia and Dr Joe de Beer published their technique on endoscopic suprascapular nerve in 2006.
Ref: Bhatia DN, de Beer JF, van Rooyen KS, du Toit DF. Arthroscopic suprascapular nerve decompression at suprascapular notch.
Suggested reading:
- Cummins CA, Messer TM, Number GW. Suprascapular nerve entrapment. J Bone Joint Surg Am 2000;82:415-24.
- Bhatia DN, de Beer JF, van Rooyen KS, du Toit DF. Arthroscopic suprascapular nerve decompression at the suprascapular notch. Arthroscopy 2006;22:1009-13.
- Lafosse L, Tomasi A. Technique for endoscopic release of suprascapular nerve entrapment at the suprascapular notch. Tech Shoulder Elbow Surg 2006;7:1-6.
- Lafosse L, Tomasi A, Corbett S, Baier G, Willems K, Gobezie R. Arthroscopic release of suprascapular nerve entrapment at the suprascapular notch: technique and preliminary results. Arthroscopy 2007;23:34-42.
- Barwood SA, Burkhart SS, Lo IK. Arthroscopic suprascapular nerve release at the suprascapular notch in a cadaveric model: An anatomic approach. Arthroscopy 2007;23:221-5.
- Poberaj B, Kovacic L. The presence of suprascapular neuropathy in rotator cuff tears. Int J Shoulder Surg 2007; in press.www.internationalshoulderjournal.org