IMPINGEMENT
Impingement is a shoulder condition found mostly in people in the 40-60 year old age group. It implies abnormal friction between the rotator cuff tendons and the overlying bone.
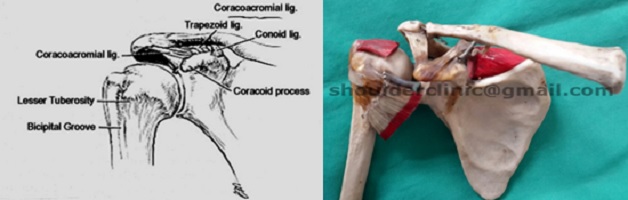
Anatomy:
The rotator cuff is the tendon belonging to the muscles, which help to elevate the arm. It passes underneath a bony roof, the acromion.
The tendons of the rotator cuff include those of the supraspinatus, infraspinatus and teres minor muscles. These tendons are collectively described as the “rotator cuff”; they run over the humeral head and insert on the greater tuberosity of the head. The muscle serves to elevate the arm. Above the tendon of the rotator cuff there is an arch consisting of bone (the acromion) and a ligament (coraco-acromial ligament).
Impingement:
The overlying acromion may squeeze or impinge upon the rotator cuff, causing inflammation and pain when elevating the arm. It is believed that, with elevation of the arm, these tendons can rub against the overlying arch and cause a condition referred to as “impingement”. Gradual overhead motion may lead to increasing impingement with swelling of the tendon, fraying out of the tendon and finally rotator cuff tears.
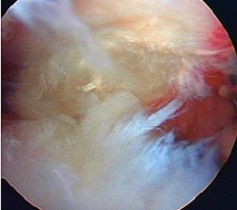

Upper structure: Acromion, Lower : Frayed rotator cuff
Symptoms:
- Painful arc: Pain when lifting the arm, usually between 40-120 degrees of elevation to the front or the side of the body.
- Pain is felt in the shoulder and down the side of the arm, aggravated by movements.
- Night pain is often a prominent feature.
Causes:
The acromion may have a prominent tip (“spur”), which could impinge on the cuff -such a spur can be seen on X-rays. Other causes may include weakness and imbalance of the surrounding stabilizing muscles of the shoulder and scapula (shoulder blade).


Treatment:
- Avoid placing the arm repeatedly in the position of impingement (overhead) till the pain has subsided.
- A stretching and strengthening programme to improve the balance of the shoulder stabilizers. This can be directed by a physiotherapist.
- Anti-inflammatory medication and other pain-relieving modalities may be used.
- Cortisone injection: The injection is placed in the space between the rotator cuff tendon and the acromion. The cortisone is mixed with local anaesthetic and the shoulder is re-examined immediately after the injection: if the pain is better the diagnosis is confirmed. The cortisone then has a local anti-inflammatory effect on the rotator cuff.
The effect of the cortisone is usually evident after 2-3 days, and the duration of the effect can vary from a few days to months.
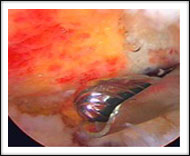
- Surgery:
If all the above fail an “acromioplasty”can be done: The acromial spur is shaved off, creating more space for the rotator cuff to glide through.
This operation should preferably be done arthroscopically (“key-hole surgery”).
The operation can be done under general or local anaesthesia. The surgeon places the arthroscope into the shoulder joint through a small 3mm skin incision. One or two similar small incisions are added to pass the instruments.
The whole joint is thoroughly checked to verify the diagnosis: at times a different problem may be found (like a tear of the rotator cuff), which was not evident during the pre-operative examination. Such a “newly discovered” problem must be dealt with there and then, using the arthroscopic technique.
If only an acromioplasty is needed, the prominent tip of the acromion is shaved off till an adequate space for the rotator cuff is created. This only takes about 20 minutes, and can be done with local or general anaesthesia. The patient can be discharged from the hospital on the same day.



Post-operative rehabilitation/ exercise programme:
After an acromioplasty an early exercise programme will be stared to regain full movement including both active and passive motion. . A shoulder sling is not needed, no limitation is placed on movements and daily activities like dressing, driving and even sport are determined by the degree of discomfort.
Full painless recovery is usually made within 4 weeks to 4 months.