The Biceps is an upper limb muscle that acts across the shoulder and elbow joints. At the elbow, it helps to bend the joint. At the shoulder, its function is more complex and incompletely understood. The biceps has two tendons around the shoulder: the long tendon passes inside the joint via a groove in the ball and attaches to the upper end of the shoulder socket, and the short tendon passes outside the joint to an adjacent bony outgrowth (coracoid).
The long tendon of the biceps is often the problematic entity in shoulder pain.
DIFFERENT DISORDERS OF THE BICEPS TENDON:
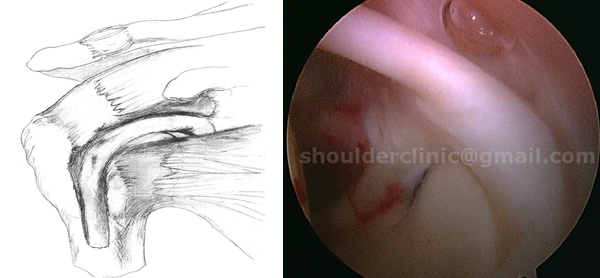
1. Inflammation of the tendon: Bicipital tendonitis
The Long tendon of the biceps slides in a groove on the shoulder ball during movements of the arm. Friction between the surfaces result in “soreness” of the tendon, called “Tendonitis”. Within the shoulder, the tendon appears “Red” with tiny blood vessels on its surface. Untreated, the tendonitis progresses to fraying and tears.
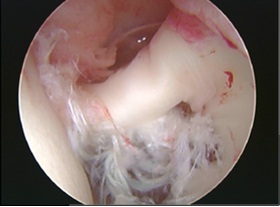
2. Fraying/ partial tearing of the tendon.
Persistence of friction on an inflamed tendon leads to this condition. The tendon appears frayed, which implies separation of individual fibres.

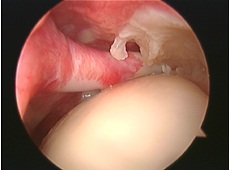
3. Complete tears/ Rupture of the tendon.
Persistence of friction on a frayed out tendon leads to this condition. The tendon cannot be seen from within the joint as it slips into the groove on the ball. The resultant slack on the muscle leads to a “Popeye” like muscle deformity.


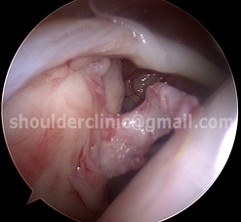
4. Tears around the tendon attachment at the upper end of the shoulder socket (arrow) are called SLAP tears . These are usually seen in throwing athletes. More information on these tears can be found under the heading “SLAP tears”.

DIAGNOSIS OF BICEPS TENDON PROBLEMS :
1. CLINICAL:
Biceps tendon disorders can present in different ways.
Pain: Pain around the front of the shoulder, arm and sometime passing down the upper limb is suggestive. The pain occurs with movements of the arm (mechanical in nature)
Clicking: Partially torn tendon and SLAP tears can cause obstruction to movements of the arm and gives an unpleasant sensation of “clicking”.
Deformity: Complete tears of the biceps tendon can result in a “Popeye” like muscle appearance.
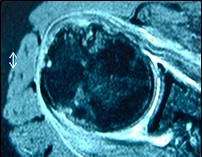
2. RADIOLOGICAL:
Xrays do not reveal biceps problems.
MRI (Right) and Ultrasound (left) are sometimes useful. Fluid around the tendon, and displacement out of the groove are some of the indicators of possible biceps pathology.

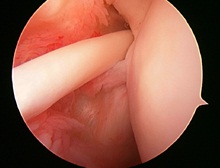
3. ARTHROSCOPY:
Arthroscopy accurately shows the inflamed, frayed, or torn biceps tendon, and SLAP tears.

TREATMENT
1. Conservative:
Avoidance of movements that cause shoulder pain.
Cortisone injections, under ultrasound control, to reduce inflammation.
Note: Conservative treatment may eliminate pain. However, there is a risk of tendon rupture with
subsequent “popeye” deformity, weakness, and cramping pain. Once ruptured, the tendon slips down the groove, and may not be reparable.
2. Keyhole surgery:
Arthroscopy identifies the problem and should be used to simultaneously treat the problem. The biceps tendon is detached from its attachment on the upper socket and is transfered to a hole created in the groove on the ball using biodegradable screws or anchors (Biceps tenodesis). This eliminates the sliding of the tendon and thereby removes friction.
Another method that can be used in elderly individuals is simply detaching the tendon from the socket and allowing it to slip down the groove (Biceps tenotomy). A cosmetic deformity and Cramping pain in the arm has been infrequently reported after this procedure.
SLAP tears are repaired, by arthroscopic techniques, to the detached area of bone using tiny anchors. Severe tears are excised and the tendon may be transferred to the groove as described above.
Often, other problems within the shoulder coexist with biceps problems. Advanced keyhole techniques allow the surgeon to identify and treat these problems simultaneously.
3. Correction of the POPEYE deformity:
Dr Deepak Bhatia has developed a minimally invasive technique to repair a POPEYE deformity. This technique is now used worldwide, and was published in the American Journal of Hand Surgery in 2012.
The technique involves a tiny incision (about 1 cm) to pull up the tendon to its correct tension, and this is then reattached to the correct position.

READ DR DEEPAK N. BHATIA ‘S SCIENTIFIC PUBLICATIONS ON THE BICEPS TENDON :
1. Bhatia DN, deBeer JF, vanRooyen KS. Direct arthroscopy of the bicipital groove: A new technique of evaluation and treatment of bicipital groove and tendon pathology. Arthroscopy. 2008; 24:368e1-e6
2. Bhatia DN, DasGupta B. Surgical correction of Popeye deformity of the Biceps Brachii muscle. J Hand Surg Am. 2012 Sep;37(9):1917-24.